December 1st, 2010 – To take adjuvant Gleevec or not take adjuvant Gleevec; this is one of the most common questions that GIST patients ask. Adjuvant Gleevec was approved by the Food & Drug Administration (FDA) for GIST in the United States in late 2008 with almost no restrictions. A few months later, it was approved by the European Commission (EC). Both of these approvals were based on results of the ACOSOG Z9001 phase III trial. Although the Z9001 trial is no longer recruiting patients, data from the trial continues to accumulate with longer follow-up of the patients in the trial.

 In presentations at the 2010 American Society of Clinical Oncologists conference (ASCO), Dr. Ronald DeMatteo, Memorial Sloan-Kettering Cancer Center (MSKCC) and Dr. Chris Corless, Oregon Health & Science University (OHSU), presented new data from the Z9001 adjuvant Gleevec trial. As Dr. DeMatteo noted, the presentations were geared towards answering two questions: Who should get adjuvant Gleevec and how long should they get it for? While the presentations went a long way towards answering who should get adjuvant Gleevec, there appears to be much that we do not know about how long they should get it for. Other ongoing trials may help shed more light on this question.
In presentations at the 2010 American Society of Clinical Oncologists conference (ASCO), Dr. Ronald DeMatteo, Memorial Sloan-Kettering Cancer Center (MSKCC) and Dr. Chris Corless, Oregon Health & Science University (OHSU), presented new data from the Z9001 adjuvant Gleevec trial. As Dr. DeMatteo noted, the presentations were geared towards answering two questions: Who should get adjuvant Gleevec and how long should they get it for? While the presentations went a long way towards answering who should get adjuvant Gleevec, there appears to be much that we do not know about how long they should get it for. Other ongoing trials may help shed more light on this question.
Who should get adjuvant Gleevec?
What’s the risk of recurrence?
Both doctors and GIST patients have developed perceptions over the years that GIST is an aggressive cancer that almost  always returns. This perception was fed by early reports of the pre- Gleevec era from GIST referral centers indicating GIST as a cancer with a very high recurrence rate after surgery, poor response rate to chemotherapy and poor survival in the case of metastatic disease. We now know that these early reports were heavily influenced by referral bias; these expert centers mostly saw the most advanced cases. Patients with smaller, less aggressive tumors were having surgery locally and in many cases were probably cured by the surgery. However, some cases of recurrence in “low-risk” tumors, sometimes as much as ten to 20 years after primary surgery, contributed to the reputation of GIST as an unpredictable, aggressive cancer.
always returns. This perception was fed by early reports of the pre- Gleevec era from GIST referral centers indicating GIST as a cancer with a very high recurrence rate after surgery, poor response rate to chemotherapy and poor survival in the case of metastatic disease. We now know that these early reports were heavily influenced by referral bias; these expert centers mostly saw the most advanced cases. Patients with smaller, less aggressive tumors were having surgery locally and in many cases were probably cured by the surgery. However, some cases of recurrence in “low-risk” tumors, sometimes as much as ten to 20 years after primary surgery, contributed to the reputation of GIST as an unpredictable, aggressive cancer.
A risk assessment was performed for the patients in the Z9001 trial. Patients were grouped according to their risk of recurrence according to the “AFIP-Miettinen” criteria. Perhaps the most surprising finding was that 44 percent of the patients were found to be at low risk of recurrence (see Table 1). Two years after entering the trial, only two percent of these patients had a recurrence. Not surprisingly, with this low rate of recurrence, there was no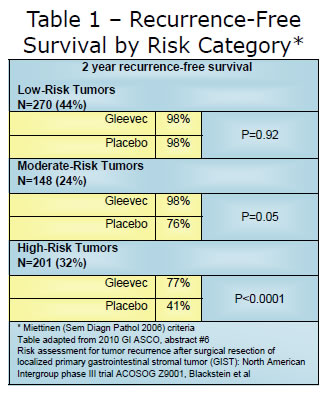 detectable difference between the placebo group and the patients that took Gleevec for a year. Although longer follow-up is needed, the early data suggests that these lowrisk patients might not require Gleevec. In contrast to the low risk group, patients at moderate and high risk of recurrence clearly had a lower rate of recurrence if they took adjuvant Gleevec.
detectable difference between the placebo group and the patients that took Gleevec for a year. Although longer follow-up is needed, the early data suggests that these lowrisk patients might not require Gleevec. In contrast to the low risk group, patients at moderate and high risk of recurrence clearly had a lower rate of recurrence if they took adjuvant Gleevec.
How is the risk of recurrence determined?
For the last several years there have been two commonly used criteria for estimating the risk of GIST tumors returning after surgery to remove a primary tumor. It’s important to understand that these methods estimate the risk only for patients that do not take adjuvant Gleevec.
The first system was developed at the GIST workshop in 2002. This system uses primary tumor size and mitotic count (also called mitotic index) to estimate the risk of recurrence. This method is especially useful when the primary tumor site is unknown. The second commonly used method is the AFIP-Miettinen method. This method was developed by Dr. Marku Miettinen and colleagues of the Armed Forces Institute ofPathology, by retrospectively analyzing several thousand cases of untreated (no Gleevec) GIST. This method adds primary tumor location to tumor size and mitotic index to determine the risk of a recurrence.
In 2009, Dr. DeMatteo and colleagues at MSKCC developed another method for determining risk of recurrence. This method is called the GIST nomogram. A nomogram is a slide rule type of estimator that assigns a point value for tumor size, tumor location and mitotic index. The points are then added to get an overall score that is used to estimate the risk of recurrence. One advantage of the GIST nomogram is that it estimates the risk at both the two-year and five-year mark. An online version of the nomogram has also been developed. This easy to use version only requires the user to input the tumor location, tumor size and check a box if the mitotic index was greater than or equal to five per 50 HPF. It will then estimate the probability of remaining recurrence-free for two years and five years. This risk is based on the patient 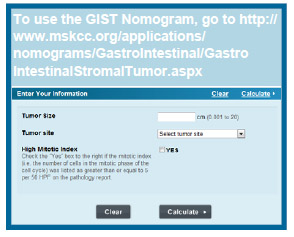 not taking Gleevec.
not taking Gleevec.
Caution: The MSKCC tool predicts recurrence-free survival (RFS), specifically, the chance a patient will survive without their cancer returning after receiving surgery alone. Recurrence-free survival as predicted by this tool has nothing to do with how long you are going to live.
In addition to tumor size, tumor location and mitotic index, Dr. Corless presented new data from the Z9001 trial that suggested patients with a KIT exon 11 deletion, especially a deletion involving codons 557-558, also had a higher risk of recurrence in the placebo group (Hazard Ratio 3.45 compared to wild-type GIST). At this time however, mutation type is not used in any the methods used to determine risk of recurrence. Tumor rupture (before or during surgery) and failure to obtain clear margins during surgery are other factors that will increase the risk of a recurrence.
Overall, a high mitotic index proved to be the greatest risk factor for recurrence for patients not taking Gleevec, with a hazard ratio of 11.3 for a mitotic rate equal to or greater than 5/50 hpf versus those with a mitotic rate below 5/50 hpf. Trial statisticians are examining whether or not a risk factor can be determined for other mitotic rates, so that risk might be related to a continuous scale rather than only above or below 5/50 hpf.
Is the patient likely to respond to Gleevec?
Mutational status has historically proven to be the best predictor of whether or not a patient will respond to Gleevec. Not surprisingly, mutational status also appears to be a powerful predictor of response to Gleevec for adjuvant treatment as well. Dr. Corless reported that in the Z9001 trial, there was a recurrence- free survival benefit for patients taking Gleevec compared to placebo for:
- Patients with KIT exon mutations (including deletions)
- Patients with PDGFRA mutations, except those with a D842V mutation.
There was no detectable benefit from Gleevec for patients with:
- Wild-type GIST (p=0.61)
- Patients with a D842V mutation.
 It should be noted that patients with the D842V mutation (which is resistant to Gleevec and Sutent) had very few recurrences (only 1) in the placebo arm or the Gleevec arm. The unanswered question was whether these patients did not have a recurrence because they had low-risk characteristics (low mitotic rate, small tumor size, etc) or whether they did not have a recurrence in spite of high-risk characteristics.
It should be noted that patients with the D842V mutation (which is resistant to Gleevec and Sutent) had very few recurrences (only 1) in the placebo arm or the Gleevec arm. The unanswered question was whether these patients did not have a recurrence because they had low-risk characteristics (low mitotic rate, small tumor size, etc) or whether they did not have a recurrence in spite of high-risk characteristics.
Dr. Corless noted that more data about adjuvant treatment was needed for those with a KIT exon 9 mutation. While there were a number of early recurrences in the placebo group and none in the first year in the Gleevec group, there was no statistical differences between the two (p=0.84), with the survival curves crossing beyond the 18 month time point. A trial to examine whether or not higher levels of Gleevec for adjuvant treatment would produce better results for exon 9 patients is in the discussion stage.
Several trials testing a longer duration of Gleevec are in progress. These trials may help answer remaining questions about adjuvant therapy including the optimal duration of therapy and whether or not adjuvant Gleevec provides a survival benefit.