
“Dear patients – I am currently sitting in a room the size of an aircraft hangar with thousands of oncologists gathered from around the world to learn and applaud the greatest improvements in your care. Progress is happening, I promise, and we are ALL rooting for you! #ASCO22” -Dr. Mark Lewis @marklewismd
For perspective – 42,600 medical professionals, graduate students, and patient advocates attended this year’s ASCO conference in Chicago (11,500 were virtual). This meeting is a beacon of hope for the cancer community.
The Life Raft Group Data Management & Research and Communications Team attended remotely to gain knowledge of current research in GIST and to track breaking news and social media networking.
General Thoughts on the Conference
According to Senior Director of Data Management & Research, Denisse Montoya, “It was fantastic to witness all the remarkable work and dedication to advanced GIST research. I know there is still a lot more to discover, but it was gratifying to know we are heading to the right direction.”
Director Sahibjeet Kaur of the Data Management Team shared her experience of the conference: “ASCO 2022 unveiled valuable data and support for continuing to push cancer research. Leading specialists from all around the world shared groundbreaking updates and insights for the benefit of patients. Being part of an advocacy organization, it was exciting and refreshing to see how much patients were put as a priority throughout the entire conference. The meeting also brought forward many new opportunities for collaborations with medical professionals and institutions to continue our mission on enhancing survival and quality of life for people living with GIST through patient-powered research, education and empowerment, and global advocacy efforts.”
Data Analyst Maeven Ludke commented, “It was amazing to witness so many enthusiastic attendees presenting and discussing ways to further advance cancer research.”
Mary Garland, Senior Director of Communications, said, “Seeing the scope of research inspired hope for the future and opens up new pathways to explore.”
And lastly, Communications Director Carolyn Tordella added, “Amazing attendance with a small conference atmosphere – we witnessed so much connection, support, and enthusiasm for the speakers and their diverse range of topics, with future intentions for collaboration and discussion amongst clinicians. It was encouraging to see so many posters and presentations on sarcoma and GIST specifically, with additional issues discussed, such as exercise for patients, advocacy and access issues, and physician burnout.”
Selected Commentaries from the Team
The team has chosen select presentations for commentary. We welcome any and all discussion and commentary. If you would like to contribute commentary or ask questions, please contact Denisse Montoya at dmontoya@liferaftgroup.org.
ctDNA
– Denisse Montoya, Senior Director, Data Management & Research – dmontoya@liferaftgroup.org
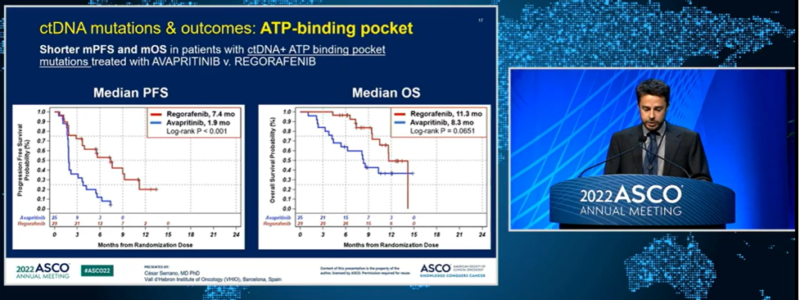 Circulating Tumor DNA (ctDNA) was a popular topic among different cancers, including GIST at the conference. Dr. César Serrano, of the Vall d’Hebron Institute of Oncology, provided a presentation about ctDNA analyses of the Phase III VOYAGER trial. The two main aims of this analysis were to explore the landscape of KIT and PDGFRA mutations in advanced GIST and to understand the role of cTDNA in measuring outcomes of patients treated with avapritinib or regorafenib.
Circulating Tumor DNA (ctDNA) was a popular topic among different cancers, including GIST at the conference. Dr. César Serrano, of the Vall d’Hebron Institute of Oncology, provided a presentation about ctDNA analyses of the Phase III VOYAGER trial. The two main aims of this analysis were to explore the landscape of KIT and PDGFRA mutations in advanced GIST and to understand the role of cTDNA in measuring outcomes of patients treated with avapritinib or regorafenib.
Baseline ctDNA analysis was performed in 386/476 patients (81%). In 333 pts (86%), ctDNA was detected with at least one gene present from the 76 they tested. 250 and 18 patients showed at least one KIT (75%) or PDGFRA (5%) variant, respectively. Dr. Serrano stated “One fourth of all KIT mutations that were detected in plasma are underreported and the predictors of pathogenicity actually showed that they were all pathogenic, which reinforced the role if ctDNA testing in this population”
The second part of the study analyzed the role of ctDNA to predict outcomes in GIST patients. Patients that had any ATP binding pocket variants detected in plasma had a lower progression free survival (PFS) when treated with avapritinib when compared to regorafenib, both with a non-significant trend in overall survival (OS). When variants in the activation loop are present in plasma, regorafenib had a higher PFS compared to avapritinib, with no significant difference in OS.
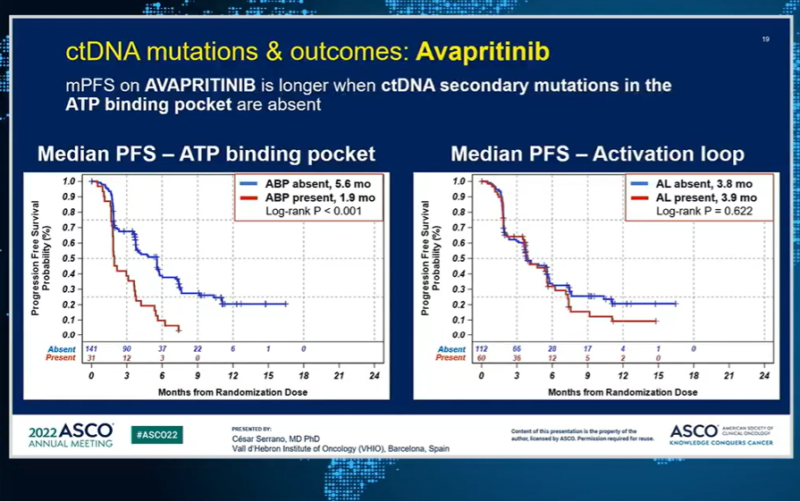
When focusing only on avapritinib, ATP binding pocket mutations are present and the PFS of avapritinib is substantially lower compared to when they are absent. However, no differences were observed on the PFS when mutations were present or absent in the activation loop. On the other hand, regorafenib was not affected by the presence or absence of mutations in the ATP binding pocket or activation loop. This confirms ctDNA as a predictor tool to the negative correlation of ATP binding pocket mutations and avapritinib.
Note: ATP binding pockets refers to mutations in exons 13 and 14 & activation loop refers to mutations in exons 17 and 18.
Abstract 101
Dr. Steve Bialick, University of Miami Miller School of Medicine/Sylvester Comprehensive Cancer Center, also presented a poster about the importance of ctDNA. The aim of the study was to analyze ctDNA from GIST patients to determine whether there is an association between certain resistance mutation and superior outcomes with different TKIs in the second line treatments and beyond. See poster here.
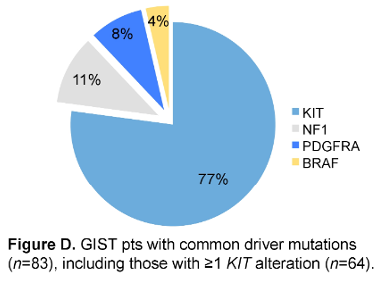 His team conducted a retrospective analysis with available ctDNA results from 104 patients who progressed on first line imatinib between 2017-2021. Driver mutations were detected in 80% (N = 83), including KIT, NF1, PDGFRA and BRAF (figure D). They identified patients with primary KIT mutations (N = 64) and known resistance mutations in KIT exons 13 (N = 25) and 17 (N = 35). 49% of patients were male with primary gastric tumors. They then studied the median time to treatment failure (mTTF) after ctDNA detection of a KIT resistant mutation for all 2L+ treatment patients.
His team conducted a retrospective analysis with available ctDNA results from 104 patients who progressed on first line imatinib between 2017-2021. Driver mutations were detected in 80% (N = 83), including KIT, NF1, PDGFRA and BRAF (figure D). They identified patients with primary KIT mutations (N = 64) and known resistance mutations in KIT exons 13 (N = 25) and 17 (N = 35). 49% of patients were male with primary gastric tumors. They then studied the median time to treatment failure (mTTF) after ctDNA detection of a KIT resistant mutation for all 2L+ treatment patients.
After a thorough analysis of the data, they were able to conclude that GIST patients with KIT exon 13 V654 resistance mutations had a superior outcome when treated in the 2L+ setting with sunitinib (mTTF= 9.6 months). They also highlighted that due to the noninvasive approach of ctDNA for detecting driver and resistance mutations, it is a potential great tool for prospective clinical trials for 2L and above in GIST patients.
Overall, both abstracts demonstrate the innovated approach of ctDNA and we are eager to see what the future of ctDNA holds for the treatment and research of GIST.
Regorafenib 3rd line therapy in advanced GISTs: A single center analysis based on different genotypes (poster)
– Director of Data Management & Research, Sahibjeet Kaur – skaur@liferaftgroup.org
Abstract 11537 – See large view of poster here.
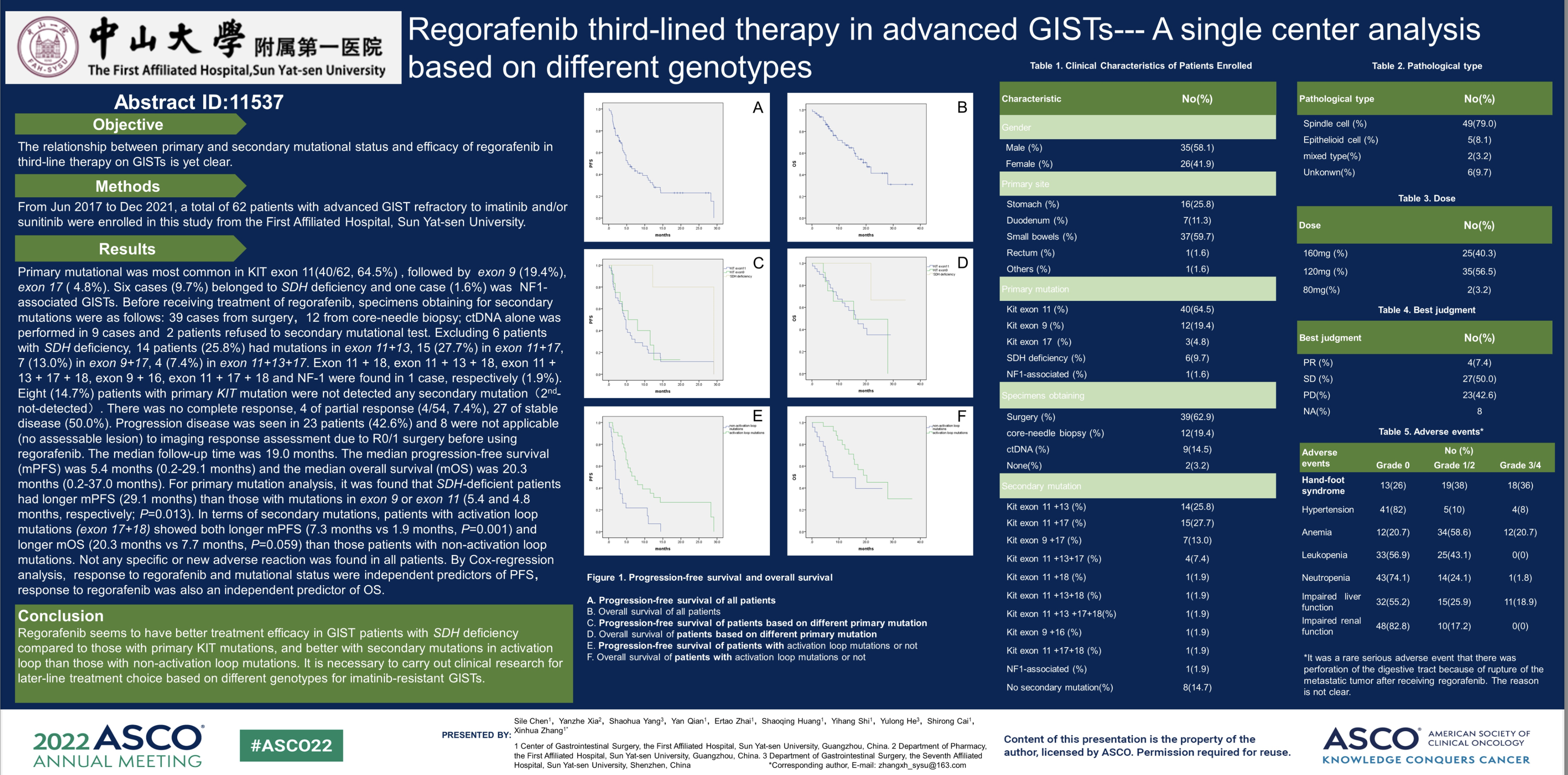
Regorafenib (branded as Stivarga) is an oral multi-kinase inhibitor approved as third line therapy for advanced and metastatic GIST. Dr. Sile Chen, PhD from The First Affiliated Hospital, Sun Yat-sen University presented a poster as ASCO 2022 looking at the relationship between primary and secondary mutation status and the efficacy of regorafenib in third-line therapy for GIST. The study was done in a single center, the First Affiliated Hospital, Sun Yat-sen University from June 2017 to December 2021 (54 months) and a total of 62 patients who had advanced GIST resistant to imatinib and/or sunitinib were enrolled.
A breakdown of the 62 patients enrolled were as followes: Kit exon 11 (64.5%), KIT exon 9 (19.4%), KIT exon 17 (4.8%), SDH deficiency (9.7%) and NF1 associated GIST (1.6%).Specimen collected to test for secondary mutations was collected prior to patients starting treatment with regorafenib. The method of obtaining the samples were as follows: 39 from surgery, 12 from core-needle biopsy, 9 from ctDNA and 2 patients refused to provide sample.
Upon testing for secondary mutation, 14 patients (25.8%) had mutations in exon 11 & 13, 15 (27.7%) in exon 11+17, 7 (13.0%) in exon 9+17, 4 (7.4%) in exon 11+13+17. Exon 11 + 18, exon 11 + 13 + 18, exon 11 + 13 + 17 + 18, exon 9 + 16, exon 11 + 17 + 18 and NF-1 was found in 1 case (1.9%). It is noted that the 6 patients with SDH deficiency were excluded.
Patients were started on regorafenib and results showed that out of 62 patients, there was no complete response recorded. 4 patients had a partial response (7.4%), 27 patients showed stable disease (50.0%). There was progression of disease in 23 patients (42.6%) and 8 patients had no assessable lesions so image response was not applicable.
Results showed that SDH deficient patients had a longer mPFS (29.1 months) than those with mutations in KIT exon 9 or 11 (5.4 and 4.8 months). Patients with activation loop secondary mutations (exon 17&18) showed longer mPFS (7.3 months) and longer mOS (20.3 months) than patients with a non-activation loop mutation (mPFS: 1.9 months; mOS: 7.7 months). Cox-regression analysis showed regorafenib response and mutation status were independent predictors to PFS and similarly, response to regorafenib was also an independent predictor of OS.
Conclusions from the study showed that regorafenib seemingly has better treatment efficacy in SDH deficient GIST patients compared to primary KIT mutations. It was also concluded from the study that better treatment efficacy with regorafenib was shown for patients with a secondary mutation in activation loop compared to those with non-activation loop mutations.
Should Mutation Status Drive Treatment Selection in Gastrointestinal Stromal Tumor?
– Data Management & Research Data Analyst, Maeven Ludke – patientregistrydepartment@liferaftgroup.org
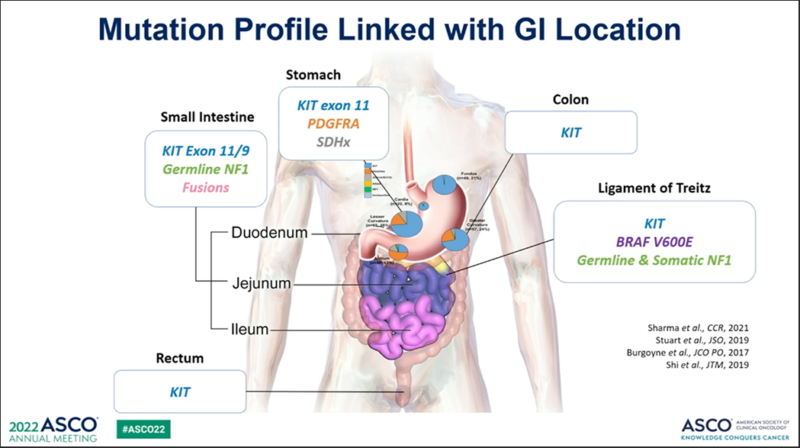 There were many great posters and presentations this year for GIST at ASCO22. One notable presentation was given by Jason Sicklick, MD, UCSD Health, discussing the role of mutational status in GIST treatments. Research continues to show the link between mutations and TKI response. While the current first through fourth line approved drugs target KIT mutations, a lot of these drugs stop working because they develop a TKI resistance from secondary KIT mutations. These can arise from GIST that has metastasized.
There were many great posters and presentations this year for GIST at ASCO22. One notable presentation was given by Jason Sicklick, MD, UCSD Health, discussing the role of mutational status in GIST treatments. Research continues to show the link between mutations and TKI response. While the current first through fourth line approved drugs target KIT mutations, a lot of these drugs stop working because they develop a TKI resistance from secondary KIT mutations. These can arise from GIST that has metastasized.
Two ways to find mutations are from testing the tumor tissue sample and from circulating tumor (CT) DNA. Studies have shown that patients respond differently to TKIs based on their mutation. Looking further into mutations and treatments, SDH-deficient GIST typically does not respond to TKI treatments. Recent treatment studies, looking at SDH-deficient GIST, have shown promising objective response rates.
Mutational testing can help doctors and patients determine which TKIs show the best response to their mutation and can help determine the best dosage for patients. This can help mitigate side effects if patients are on high doses of a treatment not shown to respond to their mutation. This not only cuts down the financial cost of the trial and error with treatments that may or may not be responsive, but it also cuts down the time cost of finding a responsive treatment. Mutational testing can significantly impact patients’ overall survival and time to progression.
Association between lung immune prognostic index, microbiome, and immunotherapy outcomes in non–small cell lung cancer
– Senior Director of Communications, Mary Garland – mgarland@liferaftgroup.org
Although there were more GIST studies this year than in years past, there were also many areas of research that could impact on the treatment of GIST patients. One such area is the field of gut microbiome. According to Dr. Jason Luke, MD, who directs the Immunotherapy and Drug Development Center at the UPMC Hillman Cancer and University of Pittsburgh, “There’s more and more evidence suggesting that there are molecular interactions between the microbiota and host immunity. A number of different mechanisms have been proposed, including modulation of myeloid cells associated with the gut lumen as well as activation of the cGAS-STING and type I interferon pathway, where good microbiota put some patients in a physiologic state where they are highly like to respond to immunotherapy.”
Studies done in non-small cell lung cancer (NSCLC) investigated this, but although it is too early to tell if the prognostic features identified link clinical evaluation of gut microbiota and the effectiveness of immunotherapy, it is a promising start. Since GIST is primarily a cancer of the gastrointestinal tract, it is logical to explore how the gut environment might influence the effectiveness of immunotherapy which is emerging as a promising treatment, including the use of FMT (Fecal Microbiota Transplant). We will be watching these developments carefully.
Link to study: https://ascopubs.org/doi/abs/10.1200/JCO.2022.40.16_suppl.9050
If you would like to contribute commentary or ask questions, please contact Denisse Montoya at dmontoya@liferaftgroup.org.
Our webinar, “Updates from ASCO,” with experts Dr. Andrew Wagner and Dr. Herbert Loong is available at: https://youtu.be/h_Jo-F926Lg


